
DIAGNOSIS
Reviewed by Dr. Anish Kapadia MD
Last updated: {insert date}
Under-diagnosis and/or misdiagnosis of a spinal CSF leak/ Spontaneous intracranial hypotension (SIH) is extremely common, resulting in little or no treatment for some patients suffering from it. Currently, there is not a single diagnostic test that can rule out SIH with a high degree of certainty; therefore, detailed assessment and investigation of symptoms by a specialist is crucial.
Possible Misdiagnosis
A CSF leak is often misdiagnosed as one of the following conditions:
Chronic migraine
Chronic tension-type headache
Chiari malformation 1
Postural orthostatic tachycardia syndrome (POTS)
Dementia (in some very rare cases)
Cervicogenic headache
New daily persistent headache (NDPH)
Meniere's disease
Post-concussion syndrome
Symptoms
Experts agree that symptoms and history of the patient are extremely important for a successful diagnosis: see SYMPTOMS.
Dr. Carroll has devised a 48-hour Flat Test to assist physicians in determining the extent to which a patient’s headache has a postural component through which symptoms improve or worsen in response to body position (horizontal vs vertical).
Neurological and Physical Examination
The results of a neurological examination are usually normal, but may show some signs related to the neurological symptoms caused by a CSF leak. These signs can vary but can include cognitive, visual, sensory, motor, balance and walking problems.
Blood Work
Blood work is usually normal in patients with CSF leaks. There is currently no routine diagnostic test on blood work for spinal CSF leaks.
Non-targeted Epidural Blood Patch (EBP)
Sustained improvement of symptoms after epidural blood patching is a good indication of a spinal CSF leak. If the initial non-targeted EBP is unsuccessful, a second, larger-volume EBP is sometimes considered, and some recommend a third lumbar or even lower thoracic level EBP before proceeding with localization of the leak with more invasive testing (i.e., CT Myelography). The success of the EBP can vary depending on the type of leak and the chronicity of the leak.
Imaging Modalities for Diagnosis
Patients with spinal CSF leak typically undergo imaging to diagnose the condition, and may require additional invasive testing, or repeat imaging/testing to make the diagnosis.
There is no diagnostic imaging test that is 100% accurate in determining whether someone is leaking. Clinicians often rely on a combination of symptoms and imaging for diagnosis and further work-up. It is important to note that MRI imaging of patients with spinal CSF leak may sometimes be normal. Spinal CSF leak can exist without any evidence of a leak on MRI imaging, and thus a negative MRI of the brain or spine does not rule out a spinal CSF leak in a patient with high clinical suspicion based on symptoms. A combination of findings from the clinical assessment and MRI imaging determines the next steps in work-up and management.
Different types of imaging include:
Brain MRI (with and without contrast) should be done in all cases where a spinal CSF leak is suspected. At a minimum, the scan should include T1 post-contrast, T2 FLAIR, and SWI (susceptibility-weighted imaging) sequences. A T2 fat-suppressed sequence through the orbits, which allows measurement of the optic nerve sheath diameter and the peri-optic subarachnoid space (the fluid-filled space surrounding the optic nerve), has also been shown to be helpful. These measurements can provide additional clues when other imaging of the brain appears normal.
There are 5 main MRI brain abnormalities which can be remembered by the acronym SEEPS:
Subdural fluid collections
Enhancement of pachymeninges (also known as dural enhancement)
Engorgement of venous structures
Pituitary hyperemia
Sagging of the brain
The brain (Bern) SIH-Score (bSIH-Score) is a quantitative scoring system of cranial MRI used to indicate the likelihood of identifying a CSF leak during more specialized spinal imaging. This scoring system relies on the six most pertinent brain MRI findings (with three major factors assigned 2 points each (pachymeningeal enhancement, venous sinus engorgement, and effacement of the suprasellar cistern ≤ 4.0 mm) and three minor factors given 1 point each (subdural fluid collection, effacement of the prepontine cistern ≤ 5.0 mm, and mamillopontine distance ≤ 6.5 mm), enabling an evaluation of the probability of a positive spinal imaging outcome in individuals with SIH ranging from 0 to 9 (higher values are associated with higher possibilities of finding a CSF leak). However, if the Bern Score suggests a low probability, patients should not be deprived of necessary evaluation and treatment if clinical suspicion remains high.
In simple terms, the Bern SIH Score is a point-based system that uses brain MRI findings to estimate how likely it is that specialized spinal imaging will find a CSF leak. A higher score means a higher chance of finding a leak. However, a low score does not mean there is no leak; clinical symptoms must always be considered.
A Full Spinal MRI (Cervical, Thoracic, Lumbar) without contrast
A heavily T2-weighted, fat-saturated, high-resolution 3D sequence, also called non-invasive MR myelography, is considered the most useful spinal imaging sequence for evaluating a suspected CSF leak. This technique provides detailed views of the spinal fluid space without requiring any injection of contrast. It allows for superior detection of subtle epidural fluid, proper assessment of the lateral epidural space (which conventional protocols often miss), and clear visualization of meningeal diverticula (small outpouchings of the dural sac along the nerve root sleeves) and nerve root sleeve cysts along the spine.
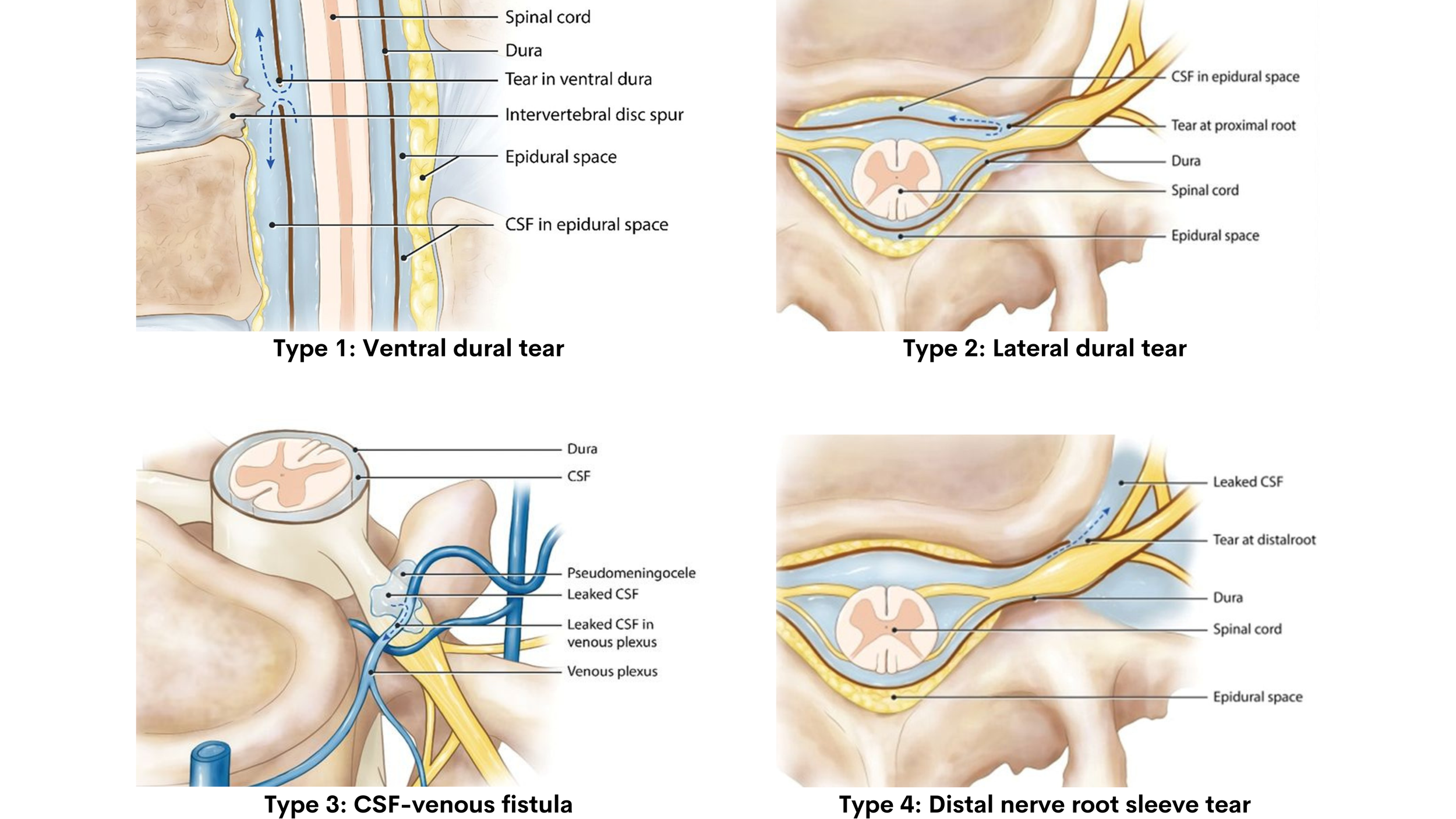
A landmark 2019 paper by Farb et al. proposed a systematic imaging approach that categorizes spinal CSF leak based on whether there is a spinal longitudinal extradural CSF collection (SLEC), a collection of CSF fluid visible along the spine on MRI. The paper identified four types of spinal CSF leaks and demonstrated that the presence or absence of SLEC is key to determining the type of leak and guiding the diagnostic and treatment approach.
SLEC-Positive (Extradural Fluid Collection Present): These patients have a visible collection of CSF outside the dural sac along the spine. This typically indicates a mechanical dural tear.
Types include:
Type 1 (Ventral Dural Tear): A tear at the front of the spinal canal, often associated with a bone spur (calcified disc or osteophyte). This is the most common type of dural tear.
Type 2 (Lateral Dural Tear): A tear occurring at the side of the dural sac, at or near the nerve root sleeve.
SLEC-Negative (No Extradural Fluid Collection): In these patients, no epidural fluid collection is visible on spinal MRI, even though brain MRI may show clear signs of intracranial hypotension.
Types include:
Type 3 (CSF-Venous Fistula (CVF)): An abnormal direct connection between the spinal subarachnoid space and an adjacent epidural vein, allowing CSF to drain directly into the venous circulation rather than pooling in the epidural space. First described in 2014, CVFs have since become an increasingly recognized cause of SIH.
Type 4 (Distal Nerve Root Sleeve Leak): A leak occurring at the far end of a nerve root sleeve. This is the rarest type identified in the study.
This systematic imaging approach using spinal MRI to first determine whether a SLEC is present predicts the nature of the underlying CSF leak and guides optimal patient positioning for myelography.
R.I. Farb et al. American Journal of Neuroradiology April 2019, 40 (4) 745-753; DOI: https://doi.org/10.3174/ajnr.A6016 (Shared with permission)
MR Myelography
MR myelography is a specialized non-invasive MRI that does not rely on the injection of contrast to view the spine. Sometimes, it can be sufficient to localize a leak, and further invasive testing is not required.
Myelography
Digital Subtraction Myelogram (DSM), and Dynamic Decubitus CT Myelography are the study of choice for locating a leak once spinal CSF leak is suspected. Both of these studies involve injection of contrast dye into the spinal subarachnoid space via a lumbar puncture. Both modalities use X-ray radiation, whereas an MRI does not involve any radiation.
Digital Subtraction Myelography (DSM)
DSM uses real-time fluoroscopy (a type of live X-ray) to take rapid images as the contrast dye flows through the spinal canal. The "digital subtraction" part means that a baseline image taken before the contrast is injected is digitally removed (subtracted) from the images taken afterward. This removes the bones and other background structures from the picture, making it much easier to see exactly where contrast dye is escaping from the spinal fluid space.
Dynamic CT Myelography
Dynamic CT Myelography is an evolving technique in which the contrast injection and imaging is performed under CT. The main advantage is its ability to provide high-resolution cross-sectional images of the anatomy.
Patient positioning during DSM and dynamic CT myelography depends on the suspected type of leak. Patients with a positive SLEC (Type 1) are best positioned prone (face down). Patients without a SLEC (Types 2, 3 and 4) are best evaluated in the lateral decubitus (lying on their side) position during myelography.
Photon-counting CT myelography (PCCT)
PCCT is a next-generation scanning technology that is thought to offer sharper image detail through higher spatial and contrast resolution, while also exposing patients to less radiation than standard dynamic CT myelography.
Cone-beam CT (CBCT) myelography
CBCT, including newer ultra-high-resolution versions, is another advancing technology that can produce highly detailed cross-sectional images and may be performed immediately after digital subtraction myelography (DSM) to confirm or further clarify findings that are uncertain.
Key Notes:
Head CT scans have low sensitivity for detecting signs of spontaneous intracranial hypotension (SIH) and are not sufficient to properly evaluate for this condition.
About 15-20% of patients with spinal CSF leak(s) have normal MRI brain imaging.
Radioisotope Cisternogram is rarely used in current practice, and it is not recommended as a diagnostic tool.
A Lumbar puncture is not a helpful diagnostic tool and is not required to make a diagnosis. The majority of patients with SIH exhibit opening CSF pressures within the normal range. A normal opening pressure does not exclude the diagnosis.
For any imaging requiring a lumbar puncture, smaller size, pencil point atraumatic type needles, versus conventional cutting needles, can minimize the risk of creating further spinal CSF leaks during testing.
While diverticula can occur in people without CSF leaks, a greater number or larger diverticula may be associated with an increased likelihood of a CSF-venous fistula. Some leaks (particularly Type 2 and Type 3) originate from or near these diverticula.
Recorded video from the 2nd Canadian SIH Conference: “MRI Brain & Spine: Findings, Bern score, Optic Nerve Sheath Diameter, Subtle Findings, Optimal Protocol.”
Recorded video from the 2nd Canadian SIH Conference: “Digital Subtraction Myelography: Utility/optimal technique for different CSF leak types, tricks and pitfalls.”
Recorded video from the 2nd Canadian SIH Conference: “Static CT Myelography, Dynamic CT Myelography & Photon Counting CT Myelography: When to use each, optimal techniques, pros and cons.”
References and Suggested Readings:
Callen AL, Fakhri M, Timpone VM, Thaker AA, Dillon WP, Shah VN. Temporal Characteristics of CSF-Venous Fistulas on Dynamic Decubitus CT Myelography: A Retrospective Multi-Institution Cohort Study. AJNR Am J Neuroradiol. 2023 Dec 29;45(1):100-104. doi: 10.3174/ajnr.A8078.
Callen AL, Pattee J, Thaker AA, Timpone VM, Zander DA, Turner R, Birlea M, Wilhour D, O'Brien C, Evan J, Grassia F, Carroll IR. Relationship of Bern Score, Spinal Elastance, and Opening Pressure in Patients With Spontaneous Intracranial Hypotension. Neurology. 2023 May 30;100(22):e2237-e2246. doi: 10.1212/WNL.0000000000207267. Epub 2023 Apr 4.
Cheema S, Anderson J, Angus-Leppan H, Armstrong P, Butteriss D, Carlton Jones L, Choi D, Chotai A, D'Antona L, Davagnanam I, Davies B, Dorman PJ, Duncan C, Ellis S, Iodice V, Joy C, Lagrata S, Mead S, Morland D, Nissen J, Pople J, Redfern N, Sayal PP, Scoffings D, Secker R, Toma AK, Trevarthen T, Walkden J, Beck J, Kranz PG, Schievink W, Wang SJ, Matharu MS. Multidisciplinary consensus guideline for the diagnosis and management of spontaneous intracranial hypotension. J Neurol Neurosurg Psychiatry. J Neurol Neurosurg Psychiatry. 2023 Oct;94(10):835-843. doi: 10.1136/jnnp-2023-331166. Epub 2023 May 5.
Dobrocky T, Nicholson P, Häni L, Mordasini P, Krings T, Brinjikji W, Cutsforth-Gregory JK, Schär R, Schankin C, Gralla J, Pereira VM, Raabe A, Farb R, Beck J, Piechowiak EI. Spontaneous intracranial hypotension: searching for the CSF leak. Lancet Neurol. 2022 Apr;21(4):369-380. doi: 10.1016/S1474-4422(21)00423-3. Epub 2022 Feb 25.
Farb RI, Nicholson PJ, Peng PW, Massicotte EM, Lay C, Krings T, terBrugge KG. Spontaneous Intracranial Hypotension: A Systematic Imaging Approach for CSF Leak Localization and Management Based on MRI and Digital Subtraction Myelography. AJNR Am J Neuroradiol. 2019 Apr;40(4):745-753. doi: 10.3174/ajnr.A6016. Epub 2019 Mar 28.
Dobrocky T, Grunder L, Breiding PS, Branca M, Limacher A, Mosimann PJ, Mordasini P, Zibold F, Haeni L, Jesse CM, Fung C, Raabe A, Ulrich CT, Gralla J, Beck J, Piechowiak EI. Assessing Spinal Cerebrospinal Fluid Leaks in Spontaneous Intracranial Hypotension With a Scoring System Based on Brain Magnetic Resonance Imaging Findings. JAMA Neurol. 2019 May 1;76(5):580-587. doi: 10.1001/jamaneurol.2018.4921.
Kranz PG, Gray L, Amrhein TJ. Spontaneous Intracranial Hypotension: 10 Myths and Misperceptions. 2018 Jul;58(7):948-959. doi: 10.1111/head.13328. Epub 2018 May 24.
Kranz PG, Malinzak MD, Gray L, Willhite J, Amrhein TJ. Resisted Inspiration Improves Visualization of CSF-Venous Fistulas in Spontaneous Intracranial Hypotension. AJNR Am J Neuroradiol. 2023 Aug;44(8):994-998. doi: 10.3174/ajnr.A7927. Epub 2023 Jul 6.
Lützen N, Zander C, Beck J, Volz F, Wolf K, El Rahal A, Urbach H. Advanced Imaging of Type 2 Spinal CSF Leaks with Ultra-High-Resolution Conebeam CT Myelography. AJNR Am J Neuroradiol. 2025 Aug 1;46(8):1736-1740. doi: 10.3174/ajnr.A8675.
Lützen N, Demerath T, Volz F, Beck J, Urbach H. Cone-Beam CT for the Detection of a Ventral Spinal CSF Leak in Spontaneous Intracranial Hypotension. Neurology. 2023 Oct 10;101(15):670-671. doi: 10.1212/WNL.0000000000207504. Epub 2023 Jul 27.
Madhavan AA, Cutsforth-Gregory JK, Brinjikji W, Bathla G, Benson JC, Diehn FE, Eckel LJ, Mark IT, Morris PP, Payne MA, Verdoorn JT, Weber NM, Yu L, Baffour F, Fletcher JG, McCollough CH. Diagnostic Performance of Decubitus Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas.AJNR Am J Neuroradiol. 2023 Dec 11;44(12):1445-1450. doi: 10.3174/ajnr.A8040.
Madhavan AA, Yu L, Brinjikji W, Cutsforth-Gregory JK, Schwartz FR, Mark IT, Benson JC, Amrhein TJ. Utility of Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas. AJNR Am J Neuroradiol. 2023 Jun;44(6):740-744. doi: 10.3174/ajnr.A7887. Epub 2023 May 18.
Madhavan AA, Cutsforth-Gregory JK, Benson JC, Brinjikji W, Mark IT, Verdoorn JT. Conebeam CT as an Adjunct to Digital Subtraction Myelography for Detection of CSF-Venous Fistulas. AJNR Am J Neuroradiol. 2023 Mar;44(3):347-350. doi: 10.3174/ajnr.A7794. Epub 2023 Feb 9.
Nath S, Koziarz A, Badhiwala JH, Alhazzani W, Jaeschke R, Sharma S, Banfield L, Shoamanesh A, Singh S, Nassiri F, Oczkowski W, Belley-Côté E, Truant R, Reddy K, Meade MO, Farrokhyar F, Bala MM, Alshamsi F, Krag M, Etxeandia-Ikobaltzeta I, Kunz R, Nishida O, Matouk C, Selim M, Rhodes A, Hawryluk G, Almenawer SA. Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. Lancet. 2018 Mar 24;391(10126):1197-1204. doi: 10.1016/S0140-6736(17)32451-0. Epub 2017 Dec 7.
Peter G. Kranz, Timothy J. Amrhein, Waleed Brinjikji, Andrew L. Callen, Ian Carroll, J. Levi Chazen, Jeremy Cutsforth-Gregory, Deborah I. Friedman, Troy A. Hutchins, Vance T. Lehman, Ajay A. Madhavan, Mark D. Mamlouk, Ian T. Mark, Marcel M. Maya, Franklin G. Moser, Simy K. Parikh, Wouter I. Schievink, Lubdha M. Shah, Vinil N. Shah, Ashesh A. Thaker, John E. Jordan. Consensus Guidelines on Diagnostic Brain and Spine Imaging of Spontaneous Intracranial Hypotension. American Journal of Neuroradiology Nov 2025, DOI: 10.3174/ajnr.A9017
Schievink WI, Maya MM, Taché RB, Prasad RS, Wadhwa V, Moser FG. Does change of spinal diverticular size predict the site of de novo recurrent CSF-venous fistulas in patients with spontaneous intracranial hypotension? AJNR Am J Neuroradiol. 2026 Feb 23:ajnr.A9258. doi: 10.3174/ajnr.A9258.
Schwartz FR, Kranz PG, Malinzak MD, Cox DN, Ria F, McCabe C, Harrawood B, Leithe LG, Samei E, Amrhein TJ. Myelography Using Energy-Integrating Detector CT Versus Photon-Counting Detector CT for Detection of CSF-Venous Fistulas in Patients With Spontaneous Intracranial Hypotension. AJR Am J Roentgenol. 2024 Apr;222(4):e2330673. doi: 10.2214/AJR.23.30673.