
Causes
Reviewed by Dr. Danny Adel Monsour, MD, FRCPC
Page last updated: May 2026

A spinal CSF leak stems from a tear or abnormality in the dura. A spinal CSF leak can occur unprovoked (called spontaneous intracranial hypotension (SIH)), may happen as a result of certain medical procedures (called “iatrogenic”) or be caused by a sudden traumatic event.
1. Spontaneous intracranial hypotension (SIH)
Common Causes of SIH
Nearly all diagnosed cases of spontaneous spinal CSF leaks fall into one of three categories.
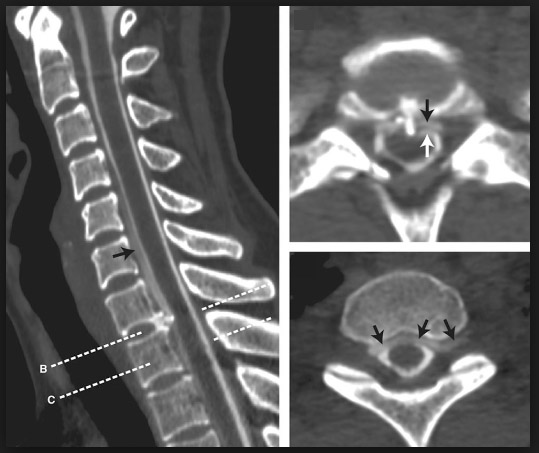
Bone-Related Tears (Type 1 Leaks) Responsible for about 25–30% of cases. Degenerative changes in the spine, such as bone spurs or calcified discs, can puncture or erode through the dura and create a direct opening in the membrane.
Nerve Root Sleeve Weakness or Tears (Types 2 & 4 Leaks) Responsible for about 30–40% of cases. These leaks arise from weakness in the nerve root sleeves, which are small extensions of the dura surrounding each spinal nerve root. Pouch-like protrusions called meningeal diverticula can form at these weak points and eventually rupture.
CSF-Venous Fistulas (Type 3 Leaks) Also responsible for about 30–40% of cases. Rather than a hole in the dura, this is an abnormal connection between the spinal fluid space and a nearby vein. Spinal fluid is siphoned directly into the bloodstream instead of leaking into the space around the spine.
Less Common Causes
In a smaller number of patients, SIH stems from more specialized conditions:
Tarlov Cysts / Sacral Dural Tears: Fluid-filled cysts near the base of the spine that occasionally become a significant source of leakage.
Sacral Dural Ectasia: Abnormal widening or stretching of the dural sac in the lower spine.
CSF-Lymphatic Fistulas: A rare condition where spinal fluid drains into the lymphatic system rather than the venous circulation or the space surrounding the spine.
Connective Tissue Disorders: Conditions such as Ehlers-Danlos Syndrome (EDS) or Marfan Syndrome can result in structurally fragile dural tissue that is more prone to leaks and fistulas.
Some predisposing factors or inciting events linked to spontaneous intracranial include:
Valsalva maneuvers:
o Heavy lifting
o Protracted coughing
o Vomiting
o Constipation/straining
Repetitive truncal tortion/twisting
o Tennis
o Golf
o Yoga
o Pialtes
o Kayaking
o Canoeing
Other
o Stretching
o Intercourse
o Chiropractic manipulation
o Roller-coaster rides
2. Medical Procedures (Iatrogenic)
Lumbar punctures, epidural catheter placement, and epidural injection. The resulting symptoms caused by unintentional dural puncture during epidural analgesia or intentional dural puncture for spinal anesthesia or for diagnostic or interventional neuraxial procedures are called Post Dural Puncture Headache (PDPH).
Spinal surgery
3. Trauma (caused by an injury)
Motor vehicle accident
Whiplash, sports-related injury
Falls
Key Notes
Some risk factors linked with a spontaneous intracranial hypotension include: Hereditary disorder of connective tissue (HDCT) such as Ehlers-Danlos syndrome, Marfan syndrome, Joint hypermobility; Spine Disorders such as Disc prolapse, Osteophytes and spondylotic spurs, Discogenic micro spurs, Dural weakness involving nerve root sleeves; Bariatric surgery.
Some experts believe that elevated pressure around the brain and spinal cord may have contributed to the leak in the first place, essentially forcing fluid through a weak point in the dura. This remains an area of active research and debate.
In many cases, PDPH is a self-limiting condition. However, in a subset of cases, PDPH can become chronic (cPDPH) or persistent (pPDPH).
After a confirmed dural puncture, for some patients, a structural change is developed, characterized by a small pseudo-meningocele or "bleb," which increases the risk of continuous cerebrospinal fluid (CSF) leakage.
Risks for PDPH can be mitigated by the routine use of noncutting (also called pencil-point or atraumatic) spinal needles, and, if using a cutting needle for an LP by using a smaller gauge needle
References and suggested readings:
Barad M, Carroll I, Reina MA, Ansari J, Flood P. Did she have an epidural? The long-term consequences of postdural puncture headache and the role of unintended dural puncture. Headache. 2021 Oct;61(9):1314-1323. doi: 10.1111/head. 14221.
Callen AL, Friedman DI, Parikh S, Rau JC, Schievink WI, Cutsforth-Gregory JK, Amrhein TJ, Haight E, Cowan RP, Barad MJ, Hah JM, Jackson T, Deline C, Buchanan AJ, Carroll I. Diagnosis and Treatment of Spontaneous Intracranial Hypotension: Role of Epidural Blood Patching.Neurol Clin Pract. 2024 Jun;14(3):e200290. doi: 10.1212/CPJ.0000000000200290.
Callen AL, Lennarson P, Carroll IR. A causative role for remote dural puncture and resultant arachnoid bleb in new daily persistent headache: a case report. Headache. 2023; 63(7): 981-983. doi:10.1111/head.14584
D'Antona L, Jaime Merchan MA, Vassiliou A, Watkins LD, Davagnanam I, Toma AK, Matharu MS. Clinical Presentation, Investigation Findings, and Treatment Outcomes of Spontaneous Intracranial Hypotension Syndrome: A Systematic Review and Meta-analysis. JAMA Neurol. 2021 Mar 1;78(3):329-337. doi: 10.1001/jamaneurol.2020.4799.
Kapan A, Waldhör T, Schiffler T, Beck J, Wöber C. Health-related quality of life, work ability and disability among individuals with persistent post-dural puncture headache. J Headache Pain. 2024 Apr 24;25(1):64. doi: 10.1186/s10194-024-01765-8.
Lützen N, Aleman EB, El Rahal A, Volz F, Fung C, Beck J, Urbach H. Sacral Dural Tears as a Cause of Spontaneous Intracranial Hypotension. Clin Neuroradiol. 2023 Dec;33(4):957-964. doi: 10.1007/s00062-023-01292-0.
Murphy, K., Nasralla, M., Pron, G. et al. Management of Tarlov cysts: an uncommon but potentially serious spinal column disease—review of the literature and experience with over 1000 referrals. Neuroradiology 66, 1–30 (2024). https://doi.org/10.1007/s00234-023-03226-6
Uppal V, Russell R, Sondekoppam R, et al. Consensus Practice Guidelines on Postdural Puncture Headache From a Multisociety, International Working Group: A Summary Report. JAMA Netw Open. 2023;6(8):e2325387. doi:10.1001/jamanetworkopen.2023.25387
Reinstein E, Pariani M, Bannykh S, Rimoin DL, Schievink WI. Connective tissue spectrum abnormalities associated with spontaneous cerebrospinal fluid leaks: a prospective study. Eur J Hum Genet. 2013 Apr;21(4):386-90. doi: 10.1038/ejhg.2012.191.
Schievink WI, Maya MM, Jean-Pierre S, Nuño M, Prasad RS, Moser FG. A classification system of spontaneous spinal CSF leaks. Neurology. 2016 Aug 16;87(7):673-9. doi: 10.1212/WNL.0000000000002986.
Schievink WI, Louy C. Precipitating factors of spontaneous spinal CSF leaks and intracranial hypotension. Neurology. 2007;69(7):700-702.
Schievink WI, Goseland A, Cunneen S. Bariatric surgery as a possible risk factor for spontaneous intracranial hypotension. Neurology. 2014;83(20):1819-1822. doi:10.1212/WNL.0000000000000985
Webb CA, Weyker PD, Zhang L, et al. Unintentional dural puncture with a Tuohy needle increases risk of chronic headache. Anesth Analg. 2012;115(1):124-132.